Root Canals, Biological Dentistry, Meridian Channels… and the Expensive Hobby of Pretending Science Is Optional
There is a particular kind of dentistry that loves to borrow the language of science while quietly avoiding its inconvenience. It speaks in a calm, serious tone about “biological harmony,” “meridian interference,” “hidden toxicity,” and the alleged danger of root canal treated teeth, as if the problem with modern healthcare is not lack of evidence, but lack of mysticism.
It is a clever performance. Dress a weak idea in technical language, add a diagram no one can verify, mention the immune system often enough, and suddenly superstition starts wearing a white coat.
The sales pitch usually goes something like this: root canal treated teeth are “dead,” they trap toxins, they silently damage the body, and they may interfere with distant organs through mysterious energy pathways called meridians. It sounds dramatic, almost enlightened. Which is precisely why it works on frightened patients.
The only problem, a minor one apparently, is that this is not how science works.
That meridian-channel idea is a perfect example. It looks deep, interconnected, like the kind of thing that must be true because it is difficult to understand and comes with arrows. But teeth are not linked to distant organs through invisible metaphysical routes waiting to be decoded by the spiritually enlightened dentist. Teeth are linked to the rest of the body through anatomy, nerves, blood supply, microbiology, inflammation, and immune response. Real biology. The unglamorous kind. The kind that does not need incense, only evidence.
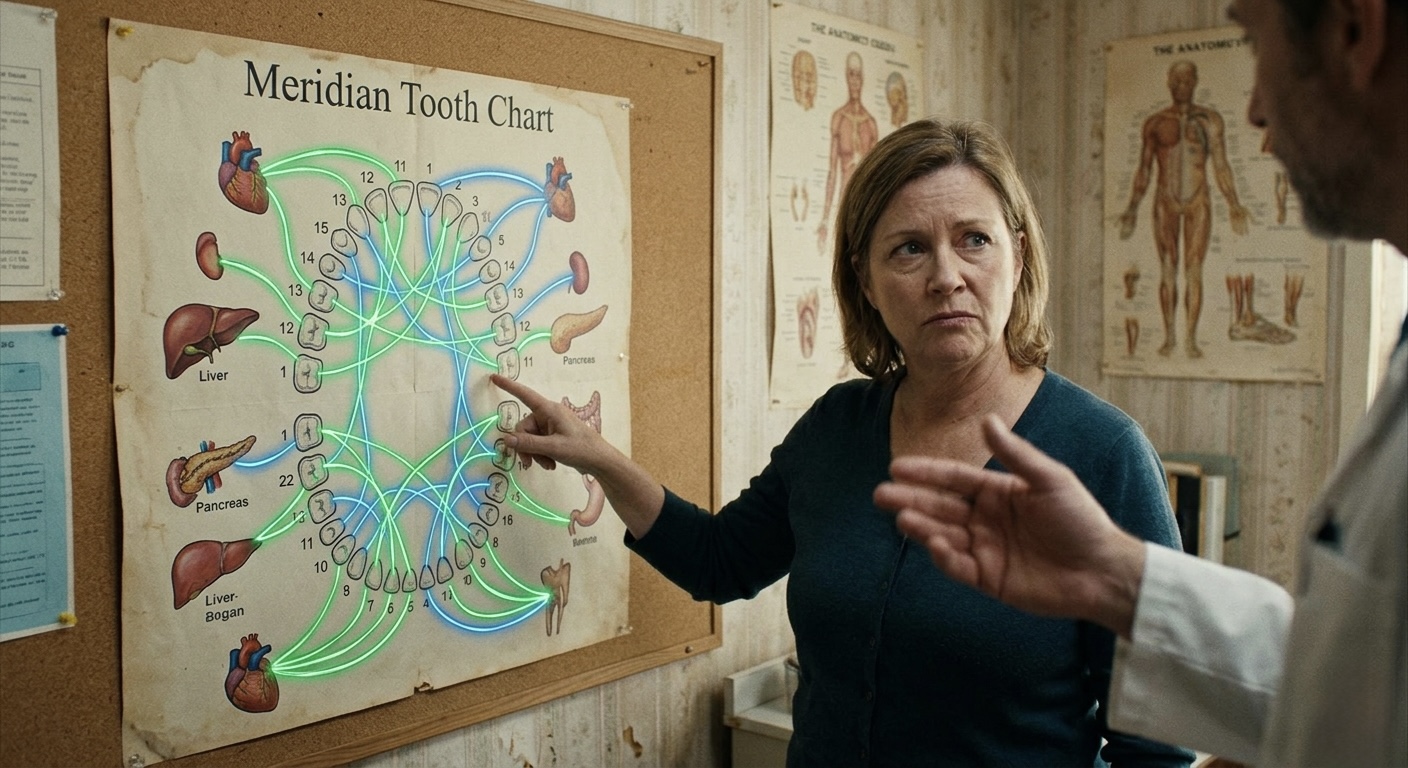
And that is the real tension here. Scientific dentistry is often less glamorous because it is forced to be honest. It has to deal with diagnosis, uncertainty, anatomy, pathology, prognosis, technical quality, restoration, follow-up, and actual outcomes. It cannot just point at a chart, lower its voice, and imply that your upper premolar is ruining your pancreas.
Modern endodontics is not based on vibes. It is based on diagnosing disease properly, eliminating infection, disinfecting the root canal system, sealing it correctly, and restoring the tooth so bacteria do not return. That is the treatment, and it works. In fact, when properly indicated and properly performed, root canal treatment is one of the most predictable and reliable ways to preserve a natural tooth. That is precisely why endodontics exists as a specialty: these cases require judgment, technical skill, and a deep understanding of pulpal and periapical disease, not mystical storytelling.
Of course, the anti-root-canal crowd rarely presents the issue that way. Fear is more profitable than honest science. “This tooth has a predictable treatment option with measurable success rates” is not nearly as lucrative as convincing a patient that their root canal treated tooth is a silent toxin factory. Once that fear is installed, the next step becomes wonderfully convenient: a more expensive replacement, usually an implant, sold as if it were a permanent upgrade beyond the limitations of nature itself. Patients are often led to believe implants are forever. They are not. Nothing in dentistry is forever. Teeth fail, root canals fail, crowns fail, implants fail, and biology has a deeply annoying habit of ignoring marketing claims.
And then we get to the evidence. Or more accurately, the abuse of the word evidence.
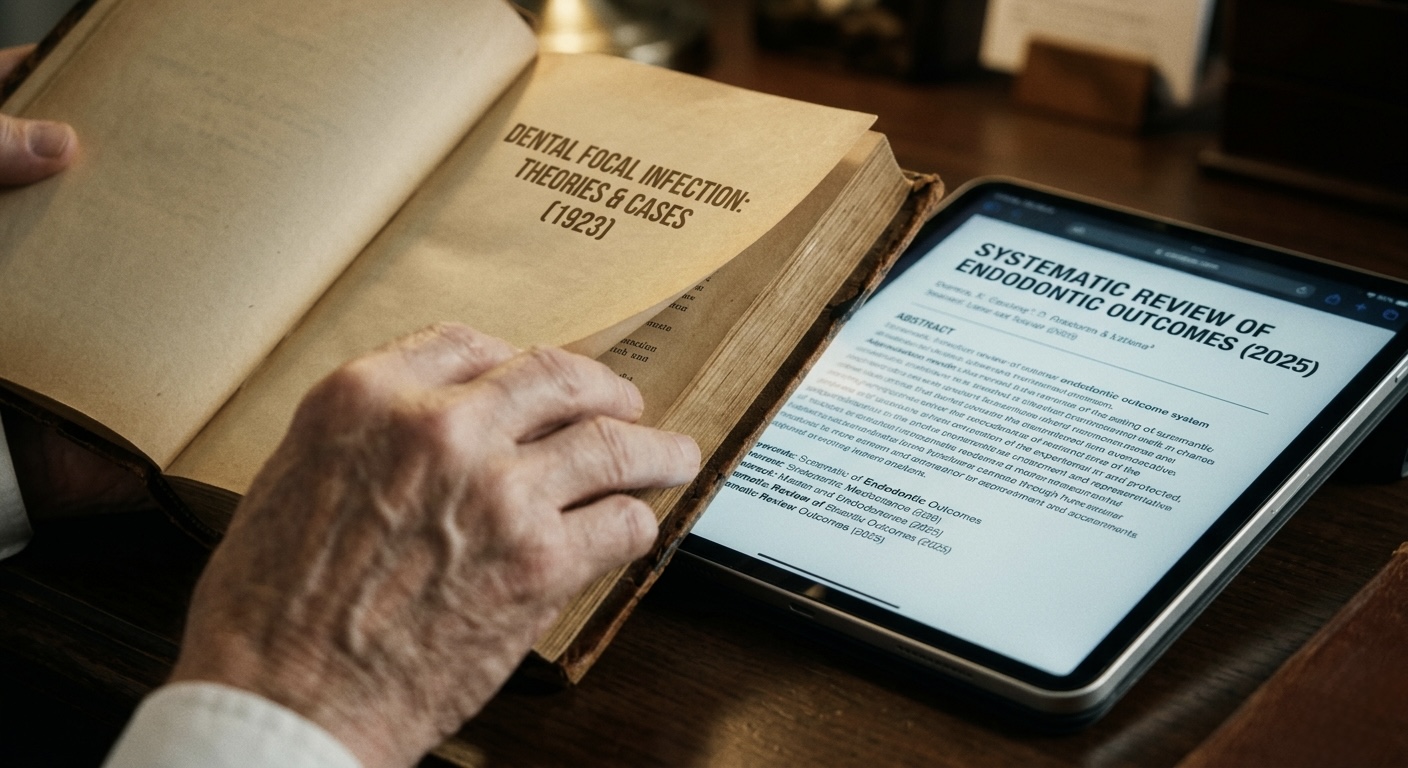
One of the oldest tricks in this space is to drag out old articles, outdated theories, isolated laboratory findings, poor-quality observational studies, or papers that are only loosely related to the claim being made, then present them as if they settle the matter. A study on bacteria? Proof that all root canals are toxic. A paper on inflammation? Proof that an endodontically treated tooth is a systemic time bomb. A historical article from another era, before modern techniques, irrigation protocols, CBCT, microscopes, adhesive restoration, and contemporary standards? Apparently still enough to terrify a patient in 2026.
This is not scholarship. It is scavenging.
Even better, some arguments lean on articles taken wildly out of context. A paper may say that oral infection can influence systemic health in certain settings, which is true and unsurprising. Then this gets twisted into: therefore every root canal treated tooth is dangerous and should be removed. That leap is not scientific reasoning. That is intellectual fraud wearing reading glasses.
And when the literature is not strong enough, there is always the magical fallback: “There are many studies.” Yes, and there are many studies on almost everything. At this point you can find an article, a preprint, a rodent model, a retrospective review, or a man with a PDF trying to prove nearly anything. Meat kills. Oxygen kills. Phones kill. Stress kills. Coffee kills. WiFi kills… Honestly, with enough determination and selective citation, even drinking water can be presented as a biochemical plot against humanity.
That is exactly why science does not work by selectively picking whatever paper flatters your preferred conclusion.
If your standard of truth is “I found an article,” then congratulations, you are one search bar away from proving the Earth is tired, bread is a neurotoxin, and socks influence liver detox. The existence of a paper is not the same as the weight of evidence. Quality matters. Context matters. Methodology matters. Reproducibility matters. Clinical relevance matters. And yes, publication date matters too, unless one’s plan is to practice dentistry like it is still 1927 but with better marketing.
This is where pseudoscientific dentistry becomes especially manipulative. It takes advantage of a very human weakness: most patients do not have the time, training, or patience to dissect literature. So if a dentist says “studies show,” shows a screenshot of an abstract, and adds a grave expression, the patient understandably assumes there must be substance behind it. Sometimes there is. Too often there is smoke, mirrors, and a bibliography assembled like a ransom note.
None of this means root canal treatment is perfect or that every tooth must be saved at all costs. That would be foolish. Some teeth are fractured. Some teeth are unrestorable. Some prior treatments are poor. Some cases fail. Retreatment may be complex. Surgery may be needed. Extraction is sometimes the correct decision. Real endodontics is not a religion. It is a discipline, it is science. It lives in the uncomfortable but respectable world of judgment.
That is the difference.
Science-based dentistry can say, “This tooth may be savable, but here are the risks, the limitations, the alternatives, and the prognosis.” Pseudoscientific dentistry prefers a cleaner story: “This tooth is toxic, your body is suffering, and I have seen what others refuse to see.” One approach respects complexity. The other flatters the ego of the speaker.
And for all the talk about being “biological,” much of this rhetoric is strangely detached from actual biology. No one seriously disputes that a necrotic, infected tooth with apical periodontitis needs treatment. The problem is the leap some make from “this tooth is infected” to “therefore it must be extracted,” as if removing a natural tooth were automatically more biological than disinfecting it, sealing it, and preserving it. Infection is real. So is overtreatment. And despite all the marketing in the world, there is still nothing better than preserving your own natural tooth whenever it can be predictably saved.
Patients deserve better than theatrical certainty wrapped in selective citations. They deserve clinicians who understand the difference between evidence and decoration, between interpretation and manipulation, between a systematic body of knowledge and a few old papers dragged out like antiques from a garage sale.
Because that is often what this comes down to: not superior science, but superior storytelling.
A root canal should never be recommended casually. But condemning root canal treatment with meridian charts, recycled myths, and cherry-picked literature is not enlightened. It is lazy. It is manipulative. And when it is used to frighten patients into irreversible decisions, it stops being eccentric and starts being irresponsible and dangerous.
If your argument needs mysticism, fossilized papers, and citation acrobatics to survive, it is not advanced dentistry. It is just superstition with a treatment plan.
PhD. MSc. Dr. Pablo Salmeron.

 Discipline is any training intended to produce a specific character or pattern of behaviour. Discipline is nothing but point a goal and achieve it through a protocol, discipline is consistency, discipline is hit the stone always in the same place, always with a good guidance of course.
Discipline is any training intended to produce a specific character or pattern of behaviour. Discipline is nothing but point a goal and achieve it through a protocol, discipline is consistency, discipline is hit the stone always in the same place, always with a good guidance of course.
 A menudo me pregunto si hacemos las cosas bien o mal, si sabiendo que las hacemos mal hacemos algo por hacerlas bien, o si sabiendo que las hacemos bien hacemos algo por intentar hacerlas aún mejor. Llegar a este punto es difícil, asumir el “se como hacerlo mejor y no lo estoy haciendo” es, cuanto menos, un asalto a viejas convicciones, costumbres y formas de hacer las cosas que, hasta ese momento, nos habían dado cierta paz interior.
A menudo me pregunto si hacemos las cosas bien o mal, si sabiendo que las hacemos mal hacemos algo por hacerlas bien, o si sabiendo que las hacemos bien hacemos algo por intentar hacerlas aún mejor. Llegar a este punto es difícil, asumir el “se como hacerlo mejor y no lo estoy haciendo” es, cuanto menos, un asalto a viejas convicciones, costumbres y formas de hacer las cosas que, hasta ese momento, nos habían dado cierta paz interior.