This case was referred to me for a re-treatment of the upper first molar with apical periodontitis. I found 5 canals. Notice the unusual location of the MB2 at the entry of the palatal canal and a DB2 next to DB canal
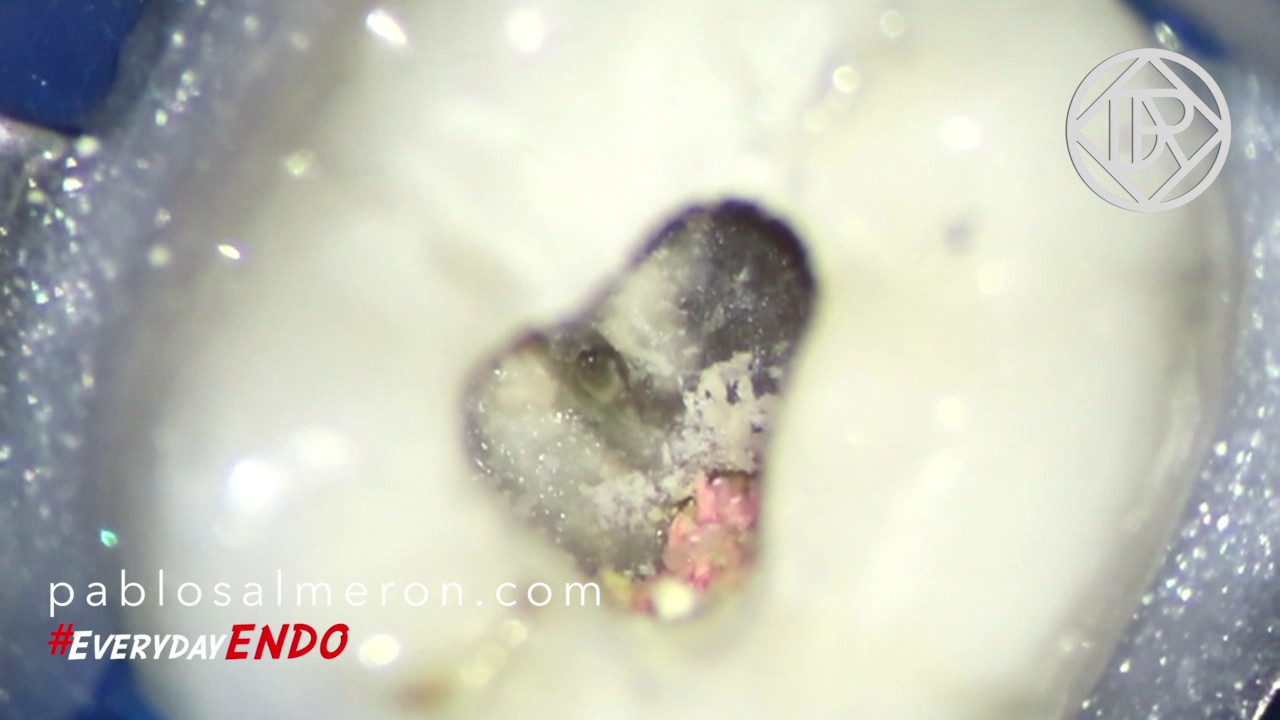
This video is about a dentin bridge I found during a root canal re-treatment of an upper seven molar. Every time I found them I like to preserve these structures to avoid tooth weakening. Only with the help of the microscope we can distinguish these kinds of formations from pulp stones. In this case the bridge was crossing the palatal canal.
What is great in man is that he is a bridge and not a goal.
The case I’m showing you today was referred to me for a re-treatment, as you can observe in the picture, there was a broken file on the distal canal with a big apical periodontitis. The treatment was planned to be done in two appointments. In the first one I removed the broken file, and placed calcium hydroxide for 25 days; In the second appointment the tooth was symptomless and I completed the treatment.
After 4 months the patient came for a review and the PA showed new bone formation, so the infection was healing.
I usually like to finish the treatments in a single appointment but is not a rule, time management has to be consider as another variable in root canals treatments and sometimes, is better to do it in two appointments and some others we need even three appointments.
Our greatest weakness lies in giving up. The most certain way to succeed is always to try just one more time.
As you can see on the video, please watch it on 720p50 HD, the case I want to show today is a re-treatment of a lower left six first molar #36. The tooth presented a ledge and missed canal on the mesial root and another ledge and a broken instrument on the distal.
Before and after
Although ledges sometimes can look easy to bypass, is not always possible to do mainly because of the location of the ledge and the patient’s opening mouth range.
Our instruments are flexible but tend to work in a straight line because their memory effect. To bypass and fix this kind of problems, we need to approach the canal in the proper angulation and as I said, sometimes is really tricky because of the limited opening range of the patient. We need to pre-bend our instrument with the proper angulation and remove dentin, as less as possible, from inside of the canal with small ultrasonic tips in order to straighten the access. A CBCT will allows us to visualize the anatomy of the root and identify the real angulation of the canal which is something we have to keep in mind when we try to bypass the ledge.
Patient, knowledge of the anatomy and the use of high magnification as the surgical microscope are the keys to success in this kind of treatments.
“Remove know from knowledge and you are standing on the ledge”.