In this post I’m going to talk about how important is to work ergonomically in dentistry and endodontics.
I like to think that modern dentistry is about details, patients nowadays are more conscious about the differences between good and bad jobs, Internet (Facebook, Youtube, Blogs…) has resulted in a great tool that has impacted on dentistry significally giving the oportunity to patients to check and investigate the perfomance of dentists before attending their practices. Patients not only research and compare differents jobs, they tend to discard all those professionals with no history on internet or those afraid to show their work fearing to be compare to other colleagues. Today, if you don’t show your work, you don’t exist.
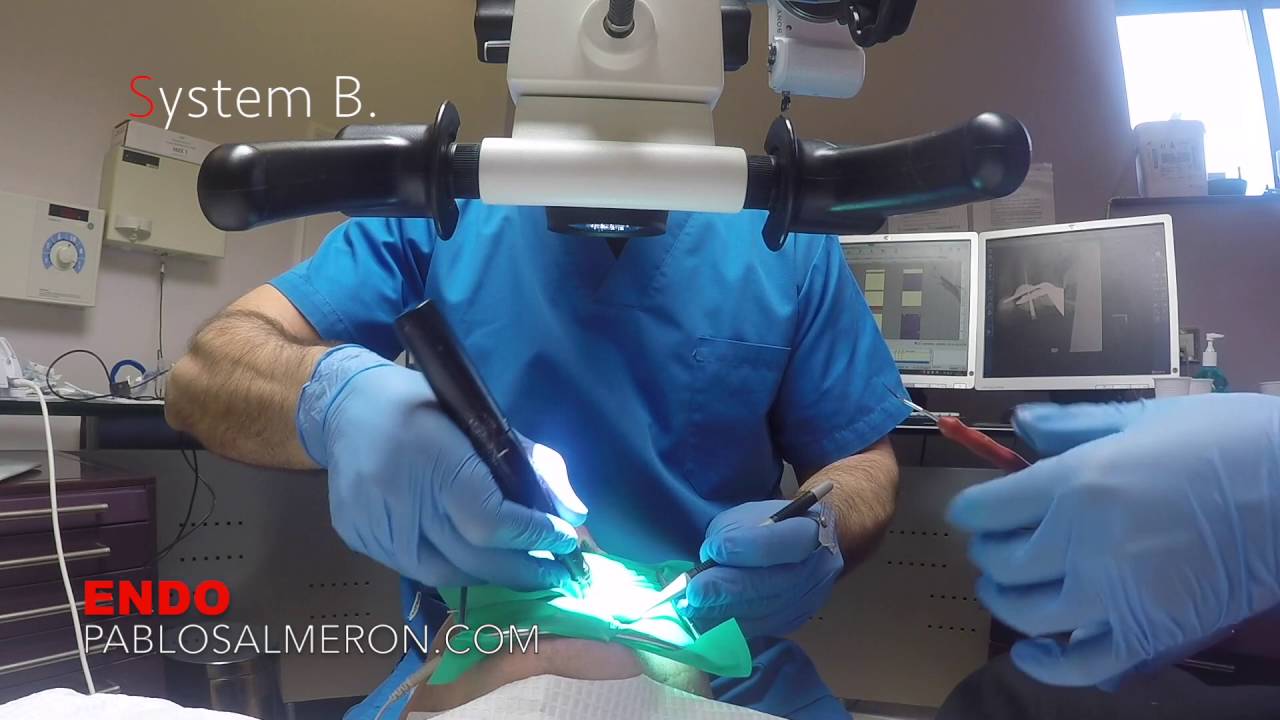
I don’t want to deviate my topic “4 handed dentistry” whit that short reflextion. Dentistry is about details and there is only one way where we’ll be able to work on it, we need to bring the object we are working with closer, that means MAGNIFICATION. “Traditional” magnification is to bend our back over the patient 90 degrees. Our eyes have some limitations to focus objects to a certain distance, more closer doesn’t mean that we see things bigger. So to be able to work on details we need to see things bigger, and there is only two solutions: 1) the use of loupes or, even better, 2) the surgical microscope. I’m not going to talk about the differences between loupes and microscopes because again that’s another topic, “Microscope is better of course :D”.
Going back to the topic, what I want to talk about is about 4 handed dentistry which, if you are able to implement little by little training your assistant, your work will radically change, letting you be more focused and relaxed doing your job, meaning, better treatments and happy patients.
So the first question we should ask ourselves is, ¿Do we need as a dentist any instrument in our side? no we don’t or at least as minimum as possible. A surgeon in an operating theatre never picks up his own instruments, the nurse do it for him, I do microsurgeries and I like to be as focused as possible on my operating field.
With the next two videos I want to show you, in a very basic way, how to pass instruments with your assistant and how you can work after some training. There is more than one technique and the location of your instruments and nurse will vary depending on your surgery setup. I hope you start and benefit implementing 4 handed dentistry in your practice.
Make it a point to do something every day that you don’t want to do. This is the golden rule for acquiring the habit of doing your duty without pain.
PhD. MSc. Dr. Pablo Salmeron.